

Rhinoplasty
Rhinoplasty is a plastic surgery procedure for correcting and reconstructing the form, restoring the functions, and aesthetically enhancing the nose and achieving the harmony of the face. It can aslo be conducted to resolve a respiratory impediment (Septoplasty, turbinectomy, polipectomy, adenoidectomy).
The operation involves modeling cartilage-and-bone support framework and soft tissues of the nose by the surgeon’s manipulations. Currently, rhinoplasty is one of the complex operations in aesthetic medicine, as the nose is the most prominent part of the face and it is almost impossible to hide nose defects. The rhinoplasty should be conducted by the surgeon who has extensive experience in the field. It is widely known that Georgia represents an endemic zone for big and Roman type of noses. Among the Soviet countries Georgia was the first to start offering nasal operations, which provided the Georgian surgeons with a strong history and experience in rhinoplasty. Through the observation of individual cases, our surgeons were able to introduce important novelties in the techniques of rhinoplasty, allowing us to achieve consistently improved outcomes. We approach each patient individually because there are no standard nasal shapes and face proportions. In each case our goal is to find a nasal shape that fits well to the facial proportions. It is also known that nasal shape can be used as an indicator of a particular character, therefore we also consider the patient’s character. The purpose of the operation is not only the making of the beautiful shape of the nose, but its harmonious alignment with the face of the patient. At the same time the nose should look natural and should have no indications of being operated on.
Primary Rhinoplasty
Indications for primary rhinoplasty are aesthetically unappealing nasal shaped – Roman nose, wide, narrow, double or asymmetric tip, and other congenital or acquired deformations. By changing the shape of the nose, you can reach harmonious facial appearance. Indications for primary rhinoplasty are also deformity in the cartilaginous septum of the nose, hypertrophy of the sidewalls, polyposis and respiratory impediments caused by adenoids. Repeated Rhinoplasty may occur is the primary surgery was not successful.
Surgery
The operation is conducted using intravenous anesthesia and it lasts for 1.5-5 hours. Incisions are hidden inside the nose, or in an open procedure, an incision is made across the columella, the narrow strip of tissue that separates the nostrils. There is no visible scar after the nasal operation. Through these incisions, the soft tissues that cover the nose are gently raised, allowing access to reshape the structure of the nose that will harmoniously fit the face. In case of respiratory impediment, the corrective surgery of cartilaginous septum of the nose takes place (septoplasty), or resection of the turbines (turbinoctomy), as well as polipectomy and adenoidectomy. In case of repeated rhinoplasty, sometimes it becomes necessary to use the transplants, which allows restoration of the nasal bone structure.
Post operation rehabilitation
After your procedure is completed, a splint, internal tubes or packing will likely be placed inside your nose for 3-6 days depending on the type of operation (aestheric rhinoplaty, septoplasty, reconstructive rhinoplasty. We use new type of packing that is easy and painless to remove. A splint or bandages is placed on the outside to support and protect the new structures during initial healing during 5-11 days. The patient is released for the hospital the second day after the operation, but remains on outpatient observation on the second, third and sixth days of the operation. The patient might experience loss of the sensitivity on the top of the nose. Patients can start driving on the third day from the operation. Full physical workload is allowed in 2 weeks from the operation. Swollen and bruised areas start to disappear in 1-2 weeks. It is not recommended to wear glasses for 2 months. The nose gets into its final shape 6-12 months from the operation, though the patient does not visibly notice small changes after the 3 weeks. Individual approach to our patients and active observation during the post-surgery period allows us to achieve consistently positive outcomes.
Technologies
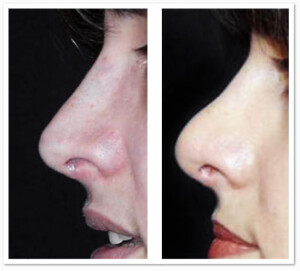
Many clinics use traditional method of rhinoplasty, without arming the bone structure of the nose. After removing the bandage, most of such patients have straight nose with small snub at the tip:

Both surgeons and the patients are happy with the results. The doctor conducts a photo session (taking photos) and their interaction ends. However, within one month, due to the incorrect fixation of the nasal tip and gravitation effect, the nose tip lowers and takes the shape of a “hawk nose”.
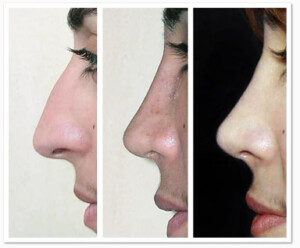
Patient after 2 weeks and 3 months of the operation.

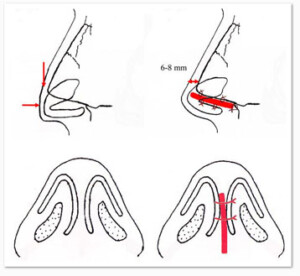
Schematic figure showing the lowring of the nose tip.
As the pictures show, the nose tip gets lowered without the reinforcement and the nose gets a beak shape.
The analysis of the rhinoplasty surgery outcomes obtained in our clinic and through the introduction of new technology in rhinoplasty – nasal tip cartilaginous skeleton reinforcement – we were able to achieve a decent aesthetic and stable results.
The goal at our clinic is is to maximize harmonious alignment of the nose with the patient’s face and personal character; At the same time it should not show any indication of the surgery and the result of the operation should be stable. To achieve this, we use the following method:
We use microsurgical method, which allows working precisely, rather than traumatologically on the soft skin tissues and nasal cartilaginous skeleton. As a result of the operation traumatism and postoperative edemas are reduced, and it is possible to obtain a good result, where traditional method would have been powerless. Any surgeon who is skilled in microsurgical techniques can successfully perform a rhinoplasty in case of nasal traumas and complex deformation cases, which many surgeons avoid to work on. For rhinoplasty we use nasal tip cartilaginous skeleton reinforcing methods, which allows us to get sustainable results and also can avoid the nose tip lowering during postoperative period and with aging.
Schematic illustration reinforcing the tip of the nose (the dock)
Patient’s image before the operation as well as 2 weeks and 3 years after the operation, which shows that nasal tip does not lower when the bone structure is framed well.
Our clinic conducts the modeling of cartilage-and-bone support framework using incision technology. Using this method, you can change a the width, length and height of the nasal tip without destruction of the cartilaginous framework.
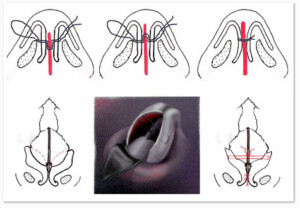
Schematic illustration of modeling nose tip.
History
It is known that rhinoplastic surgeries were conducted in India 2600 years ago. At that time in India noses were amputated as religious, criminal, or military punishment. To restore the nose a Hindu method was used which entailed the forehead flap rhinoplasty procedure that remains contemporary plastic surgical practice. However, truly aesthetic rhinoplasty was performed in 1904 by a German surgeon Jacques Joseph. He was the first to use a closed method of the operation to remove the Roman arch to a young patient who developed an inferiority complex due to the shape of the nose.

One of the students of Jacques Joseph, Gustav Aufticht, reached a perfection along with few other colleagues in the standardization of the ideal nasal shape. In the contemporary work, surgeons view “Aufricht” noses skeptically. Terms such as “standard rhinoplasty syndrome” has been introduced to refer to unnaturally narrow nose, snub nose and small and open nostrils. In the modern world, more natural nose shapes are highly demanded. The next step in the development of modern rhinoplasty was the introduction of the open operation method. The first open operation was described by Rethi in 1934, however the method only became popular in 1971, when J.R. Anderson published several articles on the open method of rhinoplasty. In the contemporary world the open methods is much more widely used than the closed method. In an open procedure one incision is made across the columella, the narrow strip of tissue, which allows modelling the nasal shape under visual monitoring. Post-operational scars are almost invisible.
The main advantages of the open method are:
- . Less traumatic pressure on the soft tissues of the nose during the incision.3. Less swelling during post-operation recovery.5. Ability to directly work on the septum, extracorporeal remodeling and further replantation on the square-shaped cartilage.7. Cartilage framework can be corrected using sutures as opposed to destructive resection. 9. Ability to detect possible deformities and asymmetries during the operation and making relevant corrections.
- 8. Ability to fixate the nasal tip, without which the outcomes of rhinoplasty can be unstable.
- 6. Using auto transplants
- 4. Ability to monitor the procedures visually, providing better opportunities for modeling the cartilage and bone support framework
- 2. Minimal loss of the blood.
Secondary Rhinoplasty
Secondary Rhinoplasty (correction of previously operated nose) and reconstructive rhinoplasty (to restore the nose shape after nose traumas or to correct congenital deformities) are much more complex operations than primary rhinoplasty as the surgeon is not aware of what was done in the first operation and what is the actual condition of the nasal bone – cartilage skeleton. Secondary and reconstructive rhinoplasty, the restoration of the nasal structures, often requires to use auto-cartilage from the nasal septum, ear or rib cartilage without damaging these donor areas. Our clinic has extensive experience in conducting such operations.
Secondary rhinoplasty often requires correction of lowered nose tip, deformed nostrils and asymmetric bone – cartilage skeleton, restoration of carved cartilage and correction of nasal deformities.
Reconstructive rhinoplasty can take place in conjunction with the surgeries of hare lip and cleft pharynx or after these operations are completed. Reconstructive rhinoplasty is used after nose injuries with the damage of internal ( bone – cartilage skeleton ) and outer (partial or complete removal of the nose) nasal structures.
During the reconstruction of nasal deformities on ( boxer ‘s nose ) is often found after the nose injury, incompetent Septoplasty (correction of curved nasal septum) and purulent nasal infection.
For nasal deformities like boxer’s nose, we see partial or complete absence of septal cartilage and loss of fixation of the nose tip. Such deformations are corrected using auto cartilage in order to restore the nasal cartilage skeleton.
Reconstruction of Deformities
During the reconstruction of nasal deformities on ( boxer ‘s nose ) is often found after the nose injury, incompetent Septoplasty (correction of curved nasal septum) and purulent nasal infection.
For nasal deformities like boxer’s nose, we see partial or complete absence of septal cartilage and loss of fixation of the nose tip. Such deformations are corrected using auto cartilage in order to restore the nasal cartilage skeleton.
Surgery
The operation is conducted using intravenous anesthesia and it lasts for 2.5-6 hours. Incisions are hidden inside the nose, or in an open procedure, an incision is made across the columella, the narrow strip of tissue that separates the nostrils. There is no visible scar after the nasal operation. Through these incisions, the soft tissues that cover the nose are gently raised, allowing access to reshape the structure of the nose that will harmoniously fit the face In case of repeated rhinoplasty, sometimes it becomes necessary to use the auto cartilage transplants from the nasal septum or rib cartilage, which allows restoration of the nasal bone structure.
Post operation period
After your procedure is completed, a splint, internal tubes or packing will likely be placed inside your nose for 3-6 weeks depending on the type of operation. We use new type of packing that is easy and painless to remove. A splint or bandages is placed on the outside to support and protect the new structures during initial healing during 5-11 days. The patient is released for the hospital the second day after the operation, but remains on outpatient observation on the second, third and sixth days of the operation. The patient might experience loss of the sensitivity on the top of the nose. Patients can start driving on the third day from the operation. Full physical workload is allowed in 2 weeks from the operation. Swelling and bruised areas start to disappear in 1-2 weeks. It is not recommended to wear glasses for 2 months. The nose gets into its final shape 6-12 months from the operation, though the patient does not visibly notice small changes after the 3 weeks. Individual approach to our patients and active observation during the post-surgery period allows us to achieve consistently positive outcomes.
Face tightening
Facelifting. Circular tightening of the face skin, tightening the upper third part of the facial skin.
Blepharoplasty
Aesthetics or upper and lower eyelids
Auriculoplasty
This is a surgical repair, restoration, or alteration of the auricle of the ear (also see reconstructive auriculoplasty). In most cases the alteration of the auricle is highly demanded due to the cupped ears. Besides the cupped ears, there are other types of defects (earlobe, anthelix and helix), which require different types of corrective procedures. Auriculoplasty does not affect the hearing.
It is widely known that sometimes cupped ears often cause complex of inferiority in children or adults. The first auriculoplasty of cupped ears was performed in 1880 by Eduard Tablot Eli in New York. The operation was performed on a 11-year old child (picture 1).
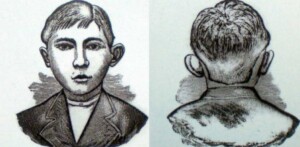
Picture 1Drawing by Eduard Tablot Eli.
In most cases the cup-shaped ears form in the first months from birth. At the age of 5, the ear shape is fully formed and auriculoplasty can be performed.
Indications
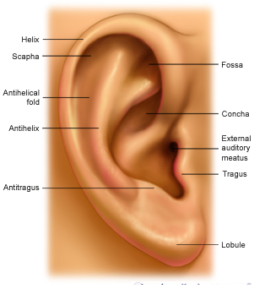
Auriculoplasty is indicated for cupped ears. Underdeveloped antihelix is also widely spread, other deformations on any part of the ear.
Operation
The operation is performed using general or local anesthesia based on the patient’s decision.
The duration of the operation is 1 – 1.5 hours.
During the operation of a cupped ear, the incision is made in the back of the year and the scar stays unnoticed after the operation. During the operation, either part of the shell is resected or fixating sutures are made. Finally excessive skin is removed and cosmetic stitches are applied.
If the operation is performed to correct the underdeveloped antihelix, the incision is made in antihelix area and the antihelix borders in the middle (medially) to the rim of the concha (shell) and the concha proper are applied special sutures, which support the formation of an antihelix.
After the surgery, the otoplasty patient wears a voluminous, non-compressive dressing upon the corrected ear(s), which should be worn for 2-3 weeks.
The patient is released from the hospital in several hours and remains on outpatient treatment.
The patients are allowed to go back to work in 2 days after the surgery.
Sutures are removed in 10-12 days after the operation. Some side effects are reduced sensitivity of ear shell and swelling for 2-3 weeks.
Final outcome of the operation is evident in 2-3 months from the surgery.
Physical activity does not need to be reduced. Scars do not stay.
Correction and Augmentation of lips
Modern plastic surgery uses several methods for correcting the shape of the lips and lip augmentation. Lip augmentation is performed by one of the two methods: using the biogradable gel and autotissiues (lip filling and auto dermal tissue).
For the reconstruction of the lip different methods are applied using the auto tissues.
Sensitive and voluminous lips always attract attention of both genders. As mentioned above there are two main methods for lip enhancement biogradable gel and auto tissue. Both have their advantages and disadvantages.
Lip enlargement gel using
Modern plastic surgery introduces bioinertive absorbable gels, hyaluronic acid, for lip augmentation. Hyaluronic acid is contained in the body and its additional insertion in the body does not have any contraindication.
At our clinic we only use modern biointertive absorbable gels for lip augmentation, manufactured by contemporary producing companies. Biopolymer, Restyline, Perlane, Martidex, Martidur, Juvederm, Purogen. All abovementioned substances contain hyaluronic acid, which is manufactured using unique technologies and differs from other substances with its biogradable nature, absorbed by the body without causing swelling of the tissues. It does not either migrate in the tissue. The natural structure of the acid changes only by 0.5-1% after insertion into the lip. The structure, sensitivity and the movement of the lip is maintained.
In the end it removes itself from the body without any trace. We select a gel for each patient based on the structure of the lip area.
Biogradable gels are used in 40 countries of the world. We are strongly against the usage of synthetic non-absorbable gels (—– and silicon), which cause a number of complications and many times lead to untreatable medical conditions or deformations.
Surgery
Lip augmentation with the bio gel fillers is not considered as a surgical procedure. The gel is inserted suing a syringe and the manipulation is performed in outpatient section of the clinic.
Post-surgery recovery
After the procedure, the patient leaves the clinic, the results can be seen immediately after the introduction of gel, the swelling will take 2-7 days. Results in 8-12 months duration. The procedure can be repeated.
Lip filling
To patients who would like to enhance lip size and maintain the outcome permanently, we offer the service of lip filling with auto tissue (lip filling and auto dermal segment).
The method uses a bodily fat, removed from the hip or abdomen area through a liposuction, which is then inserted into a lip. The procedure is performed with local anesthesia. The patient is released from the clinic in one hour after the procedure.
The negative aspect of the method is that fat tissue does not merge well with local tissues. Thus it is difficult to project how well the merging will happen and if we may have any asymmetries in the new shape of the lips.
Lip augmentation using the auto dermal segment
The tissue is obtained through an inguinal resection of upper dermal layer of the skin, which is then directly transplanted into the lips using the special channel prepared in advance.
The main advantage of the method is that it is permanent, it is safe, merges well with the tissue unlike the fat cells.
Negative side of the method is that inguinal area of resection remains with a narrow scar.
Surgery
The surgery is performed using a general or local anesthesia, depending on the emotional stability of the patient. The duration of the operation is between 30 minutes to 1 hour. After several hours the patient is released from the hospital and stays on outpatient monitoring and treatment.
Post-surgery recovery
The sutures are removed in 10-12 days.
In some cases the sensitivity of the lip area may be reduced or changed.
The patient is able to go back to work on the third day from the operation. Bruising and swelling will disappear in 1-2 weeks from the operation.
Final outcome of the surgery will be evident in 1-3 months from the operation.
Physical activity does not need to be limited.
Liposuction
This is an effective surgical method through which small incisions (0.3-0.5 cm ) are used to pump out oil from the body using the vacuum pump.
At the same time, it should be noted that liposuction is not a method used to combat obesity.
Fat accumulation predominantly occurs in genetically conditioned places ( outer tighs, buttocks, abdomen, inner thighs and chin area) and it is impossible to eliminate such fat through dietotherapy.
Some non-traditional zones for the accumulation of fat are cheeks, shoulders, and a back. Contemporary Studies revealed that local accumulation of fat in these areas do not respond to stress hormones that cause fat burning. This explains the failure of dietotherapy for body correction in these areas.
Fat tissue distribution depends on hereditary factors and gender. Losing weight results into a consequence of reduced fat tissue mass, though the contours of the body remains unchanged. Thus liposuction represents the optimal method for correcting the body shapes.
Georgia’s first suction-assisted liposuction was conducted in early 90s. In 2001, the first held ultrasound liposuction was performed. In addition to liposuction, a method or lipfilling, where the patient’s own fat is injected subcutaneously, is used.
History
The first successful liposuction was conducted in 1974 by the Italian gynecologist G. Fischer using the gynecological instruments. And the patient was his wife.
1977 Illouz and Fournier developed and used blunt cannula for liposuction. In 1985 J. Klein has developed a special solution for performing liposuction ( liposuction tumescent ) .
A pioneer in ultrasound liposuction is Zocci.
Indication
Clear indication for liposuction is a the existence of local fat clogs. Such fat clogs can be in several places together, for example.: outer thighs, buttocks, abdomen.
Surgery
The operation is mainly carried out under local anesthesia, but can be performed under general anesthesia as well. Depending on areas where the operation is conducted the duration of the surgery lasts 30 minutes – 3 hour. The incision in the skin does not exceed 0.5 cm -.
Before the surgery takes place the areas for liposuction are marked . The operation begins with entering a special solution in these zones .
Special blunt cannula , vacuum pump fat is pumped out. After the operation, the patient wears a special compressor Lingerie for 4 weeks .
The patients is transferred on outpatient treatment a few hours later.
Postoperative period
The patient can return to work 2-3 days after surgery.
Stitches are removed in 10-12 days. Sometimes loss of sensitivity can be observed temporarily in liposuction areas; as well as edemas and hemorrhage, which remain for 2-3 weeks.
In order to achieve the desired effects of the postoperative period, it is recommended to go through the rehabilitation program, the first component of the program is manual or drainage massage , especially if the skin shows marked cellulitis. The skin should be given the best possible opportunity for equal compression.
The final effect will appear 2-3 months after liposuction .
Physical activity is not restricted. Scars do not remain.
Abdominoplasty
Abdominoplasty is a surgery, which is used for the correction of the abdomen shape, reduction in volume, removal of the elasticity deformed skin in a post-natal phase, strengthening the muscles of the abdominal wall, lumbar breeding. Removal of the excess skin or fat, plastic surgery of the navel , the abdominal wall reinforcement are the essential functions of the surgery. Correction of stomach and waist contours and formation of thin scar above the pelvic bone.
For the first time in Georgia aesthetic approach to abdominoplasty was developed by our clinic staff. At present we are doing abdominoplasty operations in combination with a variety of face and body surgeries.
Starting from the 1990s we usually conduct abdominoplasty together with liposuction . These two methods complement each other, and thereby maximize the desired aesthetic result obtained. When we observe a hanging skin just below the navel , we do umbilical mini abdominoplasty without plastic procedures.
History
The first abdominal surgery to reduce the size of the abdomen was conducted by American surgeon J. held. A. Kelly (G. A. Kelly) in 1899. He used the method of dermo-lipoctemy (only removal of fatty tissue without mobilization of tissues).
In 1905, Goudet and Morestin removed a fatty tissue without excision of the umbilical and operated a hernia.
In 1916 Babcock carried out removal of fatty tissues with wide excision and tissue , which enables changing the contours of the abdomen and waist .
In 1967, the Brazilian surgeon Pitanguy was the first to describe the milestones and set new standards for the operation , which is now used to evaluate the results obtained .
These standards are: noticeable scar above the pelvic bone, sufficient mobilization of fatty segments, plastics of the navel and aponeurotic abdominal wall reinforcement.
Indications
Abdominoplasty is indicated for the correction of a hanging belly, skin aprons, excessive fat accumulation, cellulitis, distasis (separation) of abdominal muscles, umbilical, and central white line hernia. Typically these changes are associated with genetic causes, pregnancy, labor, excess weight and quick loss of weight.
Surgery
The operation is conducted under general anesthesia; the duration of the surgery is 2-5 hours. Incision is made at a bikini level. This location allows to completely cover by underwear or swimming costumes.
In case of mega abdominoplasty the incisions are made of an inverted T- shaped.
During the surgery the skin and fatty tissues are removed In case of abdominal muscle diastasis, recovery of abdominal muscle corset is completed. If the patient has a hernia it is removed during the operation.
During standard Abdominoplasty the navel is shifted and plastic procedures are applied. If the abdominoplasty corrects only the lower abdomen hanging skin mini abdominoplasty is applied without affecting the umbilical.
If necessary Abdominoplasty can be combined with liposuction of the spinal cord, thoracodorsal and other parts of the body. If the patient has lost more than 40 kg, the hanging lower abdomen skin, buttocks and thighs is evident. These are indications for body lifting (see Bariatric Surgery) . An important effect of a combined method is a compelling result with minimal post-surgical stitches and a high esthetic quality. It is necessary to wear special bandages 4 weeks after the operation. During the operation it may be necessary to use a drainage system, which is removed in 2-4 days.
Post Operation Period
Depending on the scope of surgery the patient is transferred on outpatient treatment within 3-6 days. It is possible to go back to work in 1-2 weeks after the operation. Stitches are removed in 10-12 days. In some cases temporary loss of skin sensitivity may be observed in the abdominal wall. Driving a car is allowed in two weeks.
The full extent of physical activity is allowed in 2 months. The final formation of the insicion area completes in approximately 12 months after the operation.
1. Augmentation Mammoplasty
This is an operation to increase the breast size. The purpose of the operation is to increase the size or change the shape of the breast using a silicone breast implants. It can also be used to correct light ptosis and asymmetry. Traditionally, plastic surgery for breast enlargement used one of the three main methods: Increase in size using auto tissues, injected synthetic materials and using an implant.
We conducted the first breast augmentation surgery in the 1980s , by rotating the thoracodorsal segments. It should be noted that patients at that time were very afraid of silicone implants for breast enlargement and thus could only use auto tissues.
Our clinic has been developed several methods of breast enlargement using auto tissues. As it is, this method was used in polandis syndrome (complete unilateral amastia – complete absence of a large muscle in the breast) and breast reconstruction at the time.
For our aesthetic breast surgeries our clinic uses implants from top leading firms, such as Mentor, Polytech. for implants to enlarge the world’s leading companies such as Mentor, Polytech. We prefer the augmentation through breast implants placed intramuscularly , since this method allows getting a more natural shape of the breast and much less risk of developing contractures.
–> 1.1 History
The first breast augmentation was performed by Czerny in 1995. She used tissues from the spinal cord lymphomas and transferred them to the chest to correct the asymmetry.
Later the surgeries used the tissues taken from the buttocks and the abdomen, as well as complex tissues (skin – fatty – muscle auto transplants). These methods do not give the desired results, since the transplanted tissue was desorbed and pronounced asymmetries were developed. It should be noted that at present auto tissues are widely used in breast reconstruction during oncological interventions.
The use of synthetic materials for the purpose of breast augmentation started in the 18th century. In 1899 Gersuny was the first to use the paraffin injection for breast enlargement . This was followed by the use of wax and vegetable oils, which were injected subcutaneously. Such procedures were recognized as dangerous for health and have been banned since 1960.
However, it should be noted that in some countries, unscrupulous surgeons continue to use injection liquid materials for the purpose of breast enlargement, which causes injuries of breast lymph nodes and migration of these materials into deep tissues. In such cases, it often becomes necessary to conduct the radical postmastectomy (breast removal).
Among these three methods of breast enlargement use of implants is the most justified method. The first implants were made of ivory (runs) and glass, but later rejected them because of their non-natural qualities. Subsequently the attention was focused on the Ivaloni sponge-like materials which will allow for a more natural breast shape. The use of such materials has been suspended due to complications following sponge compression, compaction, shape change, and distortion.
Evolution of modern silicone implants began in 1962, when Cronin and Gerow first used silicone implants filled with silicone gel . Over time, the silicone implant is completely expelled all other methods and materials from the practice.
Today, breast augmentation silicone implants are used in a variety of shapes and sizes. These are round, pointed and anatomical shape of the implant.
Implants can also be high- or low profile which allows the nipple – areolis be set at the desired height.
–> 1.2 Indication
Indications for augmentation can micromasty (small size of the mammary glands) , post-lactation involution (breast volume zoom out ) , delivery and breast- feeding and subsequent loss of skin elasticity, weakly expressed ptosis , and breast asymmetry. In case of pronounced ptosis , it is possible to combine the Lifting with breast augmentation.
Nowadays, as a result of many years of research, it may be safe to say that the use of implants does not increase breast cancer risk. Mammography and ultrasound examination is always an option. However, these tests are mandatory before the surgery, as well as mammalogist consultation to rule out any ongoing processes in mammary glands.
–> 1.3 Operation
The operation is carried out under general anesthesia for the duration of 1-2 hours. Dental Implants can be fixed in as intra-mammary space (under the gland), as well as a large muscle beneath the breast (IM) . The incision may be made at skin wrinkles around areolis and under the armpit. The length of the incision is 4-6 cm. During the operation the drainage system may be used, which is removed in 2-4 days.
–> 1.4 Post-operative period
Typically, patients are released and remain on an outpatient treatment from the next day. The partient can go back to work in 1 week after surgery .
Stitches are removed in 10-12 days, sometimes nipple – areolis complex experiences temporary disruption or change of senses.
Driving a car is allowed 1-2 months later.
Full physical activity allowed 2-3 months after surgery .
Complete formation of scars is over about 12 months after surgery.
2. Reproductive Mammoplasty
This is an operation to reduce the size of the breast. Its aim is to reduce the size of the breast, as well as giving a new shape and position of the breast nipple – areolis complex. The operation involves the resection of the excess breast tissue from the mammary glands. Reproductive mammoplasty had been performed at our clinic since 1990s and we use various methods of mammary gland reduction.
–> 2.1 History
Reduction of large mammary gland or the ones with ptosis was first performed y Chembers in 1896. 11 kg mass was resected , respectively.
In 1903 Guinard presented the breast reduction technique – half-oval incision was used to resect excess breast tissue and skin.
In 1928 Biesenberger provided extensive removal of breast skin and position move of the Parenchyma nipple-areolis of the breast.
In 1930, Schwarzmann first used the nipple – areolis complex nourishing and provision of adequate blood supply.
Brazilian surgeon Ivo Pitangious played a special role in reproductive Mammoplasty, who has developed several methods for this operation.
–> 2.2 Indications
Indication of reductive Mammography are large breasts, excessive sweating under the breasts, difficulty to choose linen, swimming costumes, clothing, as well as medical problems (skin irritation under skin, fatigue, pain in the back, spine diseases) .
Young patients often develop an inferiority complex because of the large breast, which makes it difficult for them to interact with their peers.
It is verified that reductive mammoplasty does not affect breast mammary gland tissue and cannot cause various types of mastopathy or cancer .
However, before the surgery, breast ultrasound or mammography examination is mandatory for all patients . Mammalogist consultation is also necessary to rule out or determine the current condition mammary glands.
–> 2.3 Operation
The operation is carried out under general anesthesia; the duration of the surgery is 3-6 hours. During the operation the excess skin, fatty tissue and part of the gland is removed. Nipple – areolis complex soft tissues are repositioned to a new place. During the operation the drainage may be applied, which is removed in 2-4 days.
–> 2.4 Post-Operative Period
The patient is usually released on written outpatient treatment in 2-3 days.
The patient can return to work within 1 week after surgery .
Stiches are removed in 10-12 days. In some cases, the nipple areolis complex may experience sensory limitations. Driving is allowed after 2 weeks .
Full physical activity is allowed in 1 month after surgery .
Complete formation of scars occurs over about 12 months after surgery . In rare cases it is possible to develop a wide range of scars and may need to be removed later.
3. Mastopexy
Lifting the mammary gland during the masto-ptosis (lowering the breast).
The aim of the operation to change the shape and position of the breast tissue by raising breast and nipple – areolis complex. Lifting is carried out mainly at the expense of the skin resection.
At hour clinic the breast lifting is performed since the beginning of 1990s. We use peri-areolar, vertical and T-like Mastopexy.
–> 3.1 History
History of breast lifting is closely related to the history of breast reduction, moreover, these operations use similar technique in many respects. The main difference lies in the fact that the incision in the skin is smaller turning the breast lifting. Also , unlike the breast reduction the skin is usually resected during breast lifting.
One of the first breast lifting operations was conducted by Michael Poussin in 1897. He made the incision above the areolis to resect part of the skin , breast and fat tissue, but the size of the breast reduced after the operation and turned unaesthetic. He was better able to reduce breast size with lifting, but the repositioning of the nipple – areolis resulted in an asymmetric arrangement.
A partial solution to this problem was found by American surgeon Max Thorek in 1921. He resected the nipple-areolis complex during lifting for tis subsequent transplantation. In modern plastic surgery medicals rejected the method of resecting the nipple – areolis complex for its subsequent transplantation.
Nowadays they perform peri-areolar, vertical and inverted T- shaped lifting. Each type of lifting has its indications depending on level of breast lowering before the operation.
–> 3.2 Indications
Indications for mastopexy derive from the such changes in the breast as expressed ptosis and limited skin elasticity due to age or breastfeeding. Mastoptozi also may develop as a result of weight loss. Mammary glands start lowering, wrinkles beneath the breast become pronounced, position of the nipples also lowers, the breast tissue moves downward, the upper contour becomes shallow, the skin is stretched.
If the patient expressed interest, the lifting can be carried out in combination with silicone breast implant augmentation. With mildly expressed ptosis, breast augmentation with silicone implant may be sufficient.
It is established that Mastopexy (Breast Lifting) does not affect the condition of breast tissue and can not cause various types of mastopathy or cancer. However, before the surgery, all patients undergo breast ultrasound or mammography examination and mammalogist’s mandatory consultation in order to verify there are no ongoing processes in the mammary glands.
–> 3.3 Operation
The operation is conducted under general anesthesia for the duration of 1-3 hours depending on the method used. Lifting occurs by repositioning of the mammary glands of the breast tissue, so that the papilla or areoli are moved to a normal position and shape of the breast is improved. Depending on the method used, the incision can be made around areoli, vertically from below the areoli or the wrinkle underneath the breast area. During the operation drainage system may be installed, which is usually removed in 2-4 days.
–> 3.4 Post-Operative period
Typically, the patient is released on outpatient treatment the second day after the surgery. The patient can return to work 3-5 days after the surgery. Stiches are removed in 10-12 days. In some cases temporary disruption or change of nipple – areolis complex sensitivity occurs. The patient is allowed to drive after 2 weeks. Full physical activity is allowed 1 month after surgery.
Complete formation of marks around incision area occurs over about 12 months after the surgery.
4. Asymmetry of Mammary Glands
Asymmetry can originate from both congenital diseases, for example polandis syndrome, as well as the usual asymmetry. Various methods can be used to correct breast asymmetry: breast endo-protesis, breast lifting along with endo-protesis, reductive mammoplasty.
Correction of Face Contours
Correction of face shapes and ovals, correcting the defects
Body Lifting
Bariatric surgery falls under the competence of Abdominal Surgeons. After these operations, the patient loses weight which results in the development of soft tissue ptosis (suspension). After the stabilization of body weight, plastic surgeons get intolved to correct body shapes with the following types of surgeries: body lifting, breast lifting-reduction, lifting buttocks, hips, shoulder and etc.
Indications
Indications for Body lifting are the affects of massive weight loss where after the bodily skin usually lowers in the abdomen area, around the buttocks, hips, shoulders, breast and other. Operation is designed to allow the skin stretching.
Operation
The operation is carried out under general anesthesia, duration of the operation is 1,5-6 hours. Skin stretching is carried out in stages. At the first stage stretching the skin of the buttocks and abdomen is performed, in the next place the thighs, shoulders and breast skin stretching is performed. During the operation excess skin in removed , stretched and fixed to get stable good results . During the operation drainage system may be set, which is removed within 2-12 days after the operation.
Post-Operative period
The patient is usually released on outpatient treatment within 7-12 days after the surgery. The patient can return to work in 3 weeks.
Stitches are removed in 10-12 days after the operation. In some cases temporary disruption or change of nipple – areolis complex sensitivity occurs. The patient is allowed to drive after 3 weeks. Full physical activity is allowed 3 month after surgery.
Complete formation of marks around incision area occur over about 12 months after the surgery.
In some cases, the nipple may occur – areolis complex sensory disturbance or change . Driving is allowed after 3 weeks .
Complete physical load allowed 3 months after surgery .
Complete formation of scars over about 12 months after surgery . In rare cases it is possible to develop a wide range of scars and may need to be removed later .
Correction of Buttocks
Correction of Shin
Correction of Shin using the implants.